Intraoperative Neuromonitoring (IONM)
Intraoperative neuromonitoring refers to the techniques used to monitor nerve function during a surgery. The exact nerve monitored depends on the nerve at risk during the surgical procedure. For thyroid and parathyroid procedures, the laryngeal nerves are at risk of injury (the recurrent laryngeal nerve and the external branch of the superior laryngeal nerve). For parotid and submandibular gland surgery, the facial nerve is at risk of injury. A/Prof Sinclair is highly experienced in IONM techniques and utilizes this technology with all thyroid, parathyroid and salivary gland operations. She has published and lectured widely on these techniques and have innovated and developed a stand-alone technique for continuous IONM of the laryngeal nerves during thyroid / parathyroid surgery (see below).
IONM during thyroid and parathyroid surgery
The thyroid and parathyroid glands sit in a tight pocket in the middle of the neck, surrounded by critical structures such as the airway, esophagus and laryngeal nerves. The recurrent laryngeal nerves (RLN) supply the interior muscles of the voice box to move the vocal folds during speech and singing. The EBSLN supplies a muscle that sits on the outside of the voice box, directly under the thyroid gland, called the cricothyroid muscle. This muscle is essential for raising the pitch of the voice and its function is indispensable for singers and professional voice users.
The RLN can be monitored by two techniques. One, termed ‘intermittent IONM’, uses intermittent direct nerve stimulation with a hand-held probe to assess nerve function at various times during a surgery (as determined by the operating surgeon). Unfortunately, this type of monitoring does not provide ‘real-time’ feedback regarding nerve function and thus the nerve can be injured in between the surgeon-determined stimulations. The other form of monitoring is called ‘continuous IONM’. This method provides real-time feedback about nerve function every second of the surgery and thus evolving nerve injury can be recognized early and reversed. As such, this technique can truly prevent slowly evolving nerve injuries during thyroid and parathyroid surgery. Unfortunately, continuous IONM is rarely performed by surgeons in Australia. A/Prof Sinclair is a world leader in continuous IONM and, in 2016, developed a new, non-invasive method for monitoring the RLN which is called LAR-CIONM. She has published and lectured widely on this technique, which is now being developed in Germany for worldwide use. She is very pleased to introduce this technology into Australia.
A/Prof Sinclair often refers to the EBSLN as ‘the forgotten nerve of thyroid surgery’. Recent studies suggest that this nerve is frequently injured in thyroid operations and that the rates of injury have been grossly under-reported. Pleasingly, rates of injury can be drastically reduced by implementing IONM of the EBSLN. However, few surgeons routinely monitor this nerve. A/Prof has lectured widely on the benefits of IONM of the EBSLN and is a strong proponent for universal adoption of EBSLN IONM. She utilized EBSLN IONM for all thyroid surgeries.
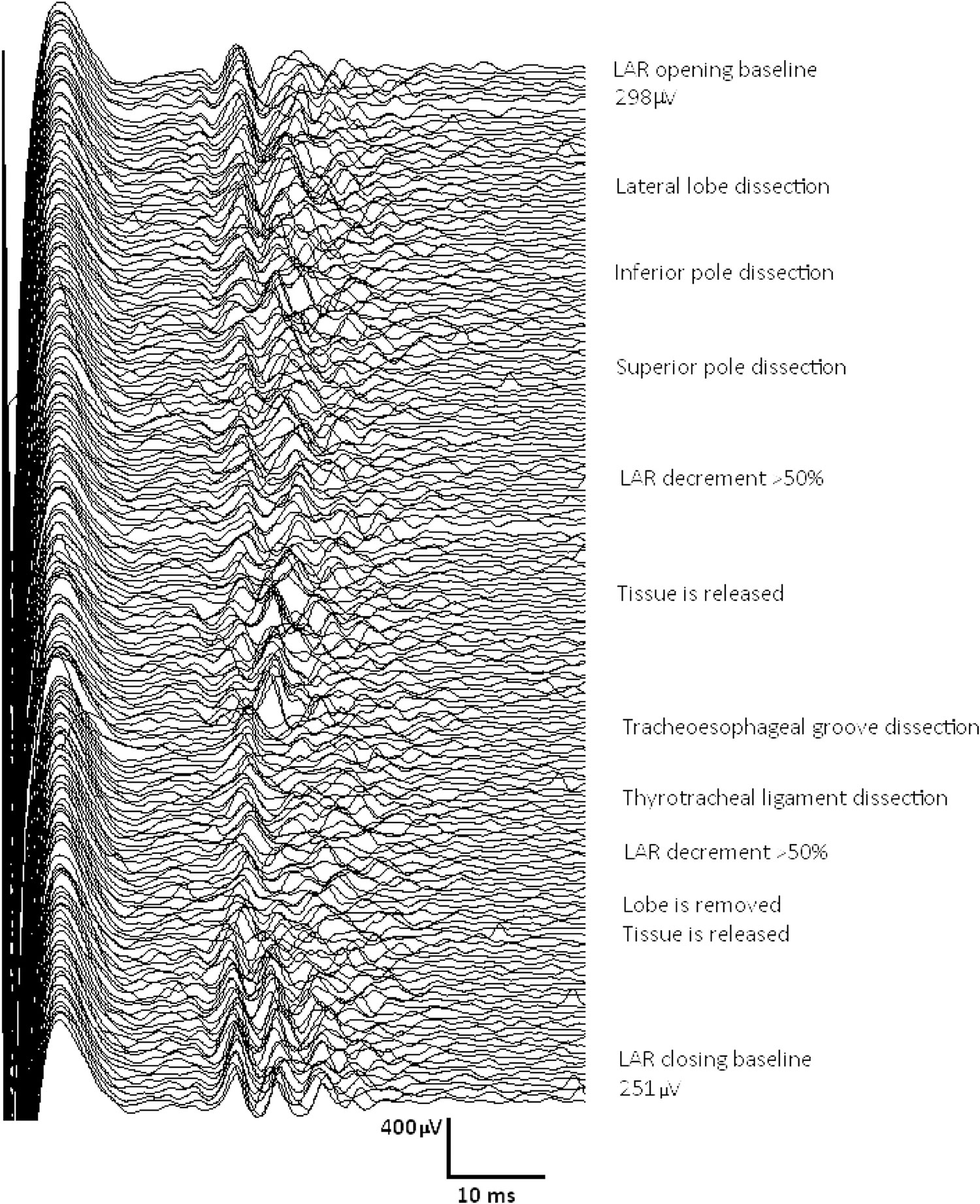
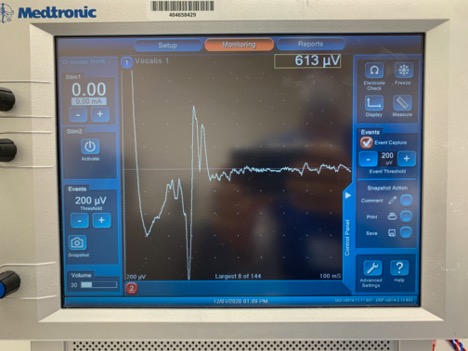
Figure: An example of the type of real time feedback obtained with LAR-CIONM during a thyroid surgery